Is The Future of Psychiatry Scientific?

Imagine for a moment that the American Psychiatric Association was about to compile a new edition of its Diagnostic and Statistical Manual of Mental Disorders but instead of 2019, the year is 1880.
Transported to the world of the late 19th century, our nation’s preeminent psychiatric body would have virtually no choice but to include hysteria in the pages of its new volume. At the turn of the last century, women by the tens of thousands, after all, displayed the distinctive signs: convulsive fits, facial tics, spinal irritation, sensitivity to touch, and leg paralysis. Not a doctor in the Western world at the time would have failed to recognize the presentation. “The illness of our age is hysteria,” a French journalist wrote. “Everywhere one rubs elbows with it.”
Hysteria would have had to be included in our hypothetical 1880 DSM for the exact same reasons that attention deficit hyperactivity disorder is included in the recently released DSM-5. The disorder clearly existed in a population and could be reliably distinguished, by experts and clinicians, from other constellations of symptoms. There were no reliable medical tests to distinguish hysteria from other illnesses then; the same is true of the disorders listed in the DSM-5 today. Practically speaking, the criteria by which something is declared a mental illness are virtually the same now as they were over a hundred years ago.
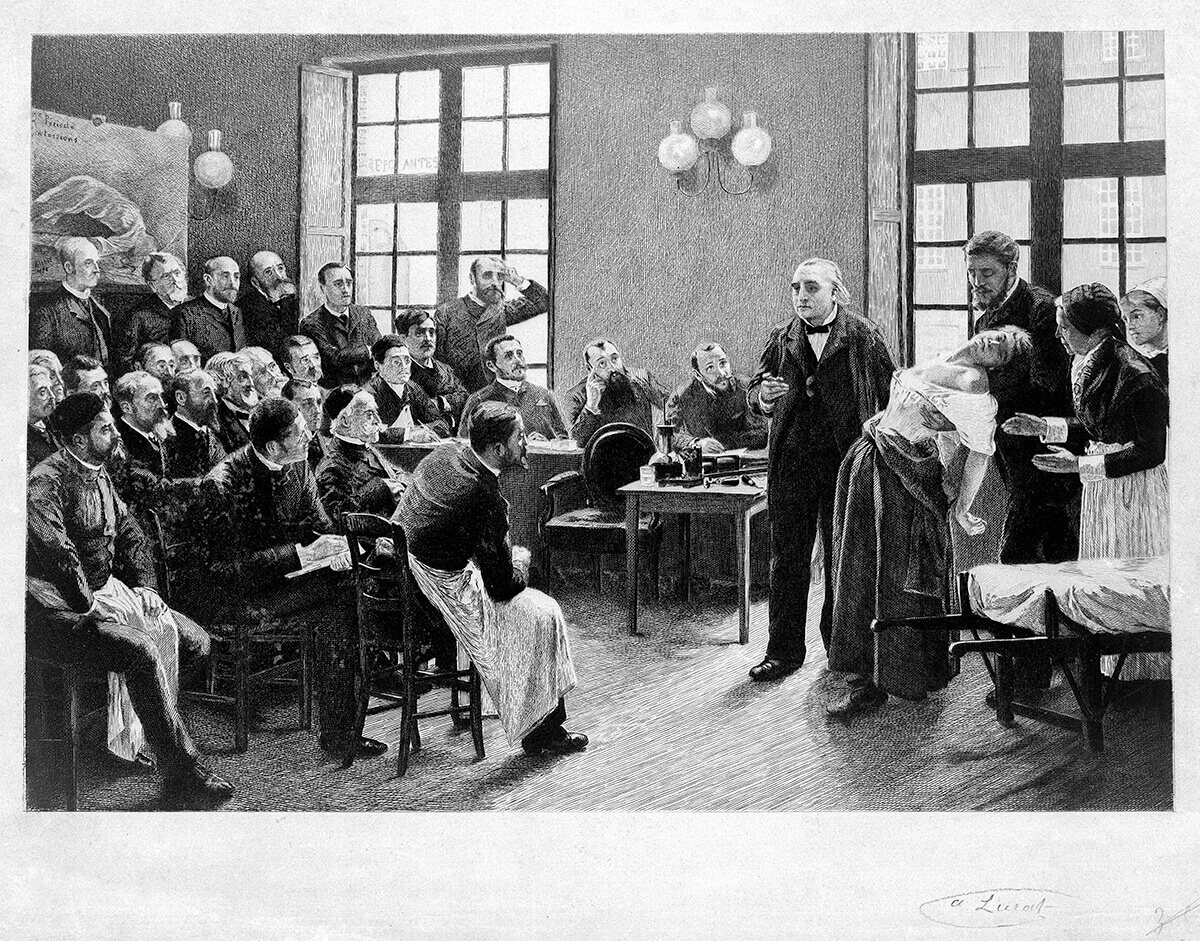

Jean-Martin Charcot demonstrating hysteria in a patient at the Salpetriere. This image from Wellcome Images.
…the DSM diagnoses are based on a consensus about clusters of clinical symptoms, not any objective laboratory measure. In the rest of medicine, this would be equivalent to creating diagnostic systems based on the nature of chest pain or the quality of fever.
Thomas R. Insel, M.D.Former Director, National Center for Advancing Translational Sciences, Director, National Institute of Mental Health

Recently, a large study suggested that 46 percent of Americans will receive a mental-health diagnosis at some point in their lifetimes. Critics like Frances suggest that, with the new categories and loosened criteria in the DSM-5, the percentage of Americans thinking of themselves as mentally ill will rise far above that mark.


But recent history doesn’t support these fears. In 1994 the DSM-IV—the edition Frances oversaw—launched several new diagnostic categories that became hugely popular among clinicians and the public (bipolar II, attention deficit hyperactivity disorder, and social phobia, to name a few), but the number of people receiving a mental-health diagnosis did not go up between 1994 and 2005. In fact, as psychologist Gary Greenberg, author of The Book of Woe, recently pointed out to me, the prevalence of mental health diagnoses actually went down slightly. This suggests that the declarations of the APA don’t have the power to create legions of mentally ill people by fiat, but rather that the number of people who struggle with their own minds stays somewhat constant.
What changes, it seems, is that they get categorized differently depending on the cultural landscape of the moment. Those walking worried who would have accepted the ubiquitous label of “anxiety” in the 1970s would accept the label of depression that rose to prominence in the late 1980s and the 1990s, and many in the same group might today think of themselves as having social anxiety disorder or ADHD.
Viewed over history, mental health symptoms begin to look less like immutable biological facts and more like a kind of language. Someone in need of communicating his or her inchoate psychological pain has a limited vocabulary of symptoms to choose from. From a distance, we can see how the flawed certainties of Victorian-era healers created a sense of inevitability around the symptoms of hysteria. There is no reason to believe that the same isn’t happening today. Healers have theories about how the mind functions and then discover the symptoms that conform to those theories. Because patients usually seek help when they are in need of guidance about the workings of their minds, they are uniquely susceptible to being influenced by the psychiatric certainties of the moment. There is really no getting around this dynamic. Even Insel’s supposedly objective laboratory scientists would, no doubt, inadvertently define which symptoms our troubled minds gravitate toward. The human unconscious is adept at speaking the language of distress that will be understood.
Journalists play a role as well: We love to broadcast new mental-health epidemics. The dramatic rise of bulimia in the United Kingdom neatly coincided with the media frenzy surrounding the rumors and subsequent revelation that Princess Di suffered from the condition. Similarly, an American form of anorexia hit Hong Kong in the mid-1990s just after a wave of local media coverage brought attention to the disorder.
The trick is not to scrub culture from the study of mental illness but to understand how the unconscious takes cues from its social settings. This knowledge won’t make mental illnesses vanish (Americans, for some reason, find it particularly difficult to grasp that mental illnesses are absolutely real and culturally shaped at the same time). But it might discourage healers from leaping from one trendy diagnosis to the next. As things stand, we have little defense against such enthusiasms. “We are always just one blockbuster movie and some weekend therapist’s workshops away from a new fad,” Frances writes. “Look for another epidemic beginning in a decade or two as a new generation of therapists forgets the lessons of the past.” Given all the players stirring these cultural currents, I’d make a sizable bet that we won’t have to wait nearly that long.