
Hearts Afire

A handful of studies focusing on firefighters’ cardiac responses to stress show within 15 seconds after an alarm sounds, heart rates soar 61 beats per minute on average. While resting, our heart beats about 60 to 70 times each minute. Therefore, the heart rate nearly doubles within 15 seconds of an alarm. Athletes in training usually get 15 minutes of warm-ups to raise heart beats that high.
An analysis of data in those studies shows:
- Firefighting raises the threshold for heart attacks, ischemia/angina and stroke;
- Age is a significant factor in heart attacks, but not the only one;
- Alarm systems, or Klaxons, may well contribute over time to heart trouble;
- Alarms provide just as stressful when false as when real;
- Firefighters arrive at emergencies with heart pumping at 88 percent of capacity. In other words, systolic pressure, indicating the pressure during the heart’s initial contraction (the upper number of a blood-pressure reading) remains at 80 to 100 percent capacity until the emergency ends, sometimes hours later;
- We need more studies to address health issues facing firefighters, particularly cardiovascular fitness.
Figure 1: 1998 Line of Duty Deaths by Type
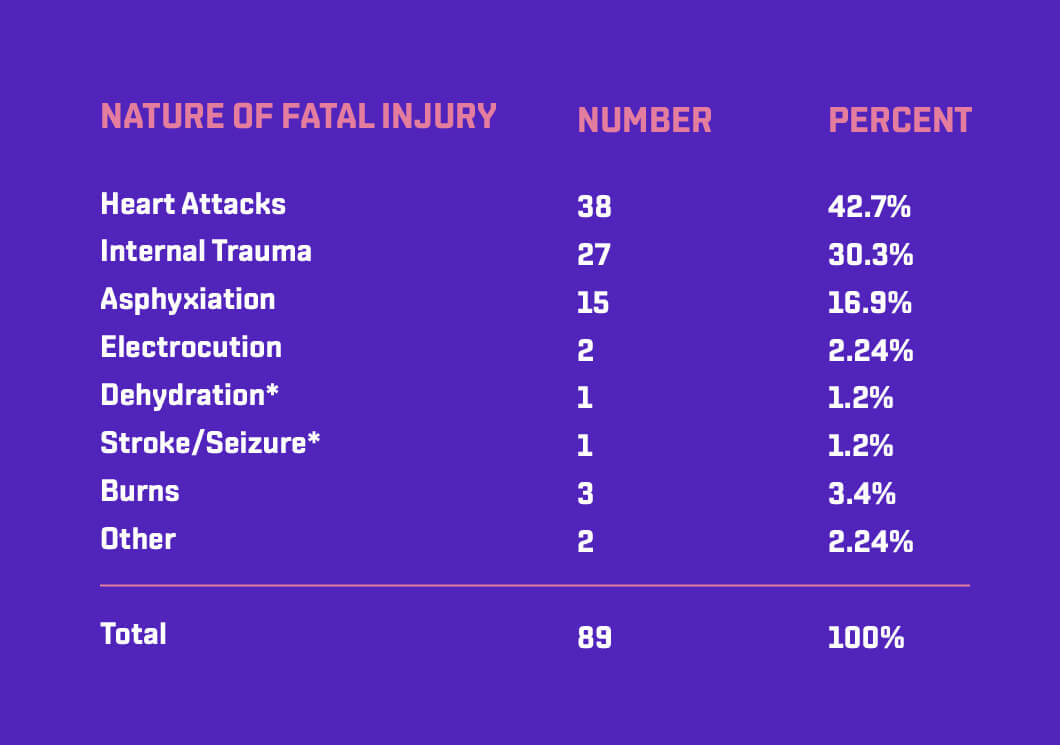

Figure 2: Firefighter Deaths and Injuries, 1994
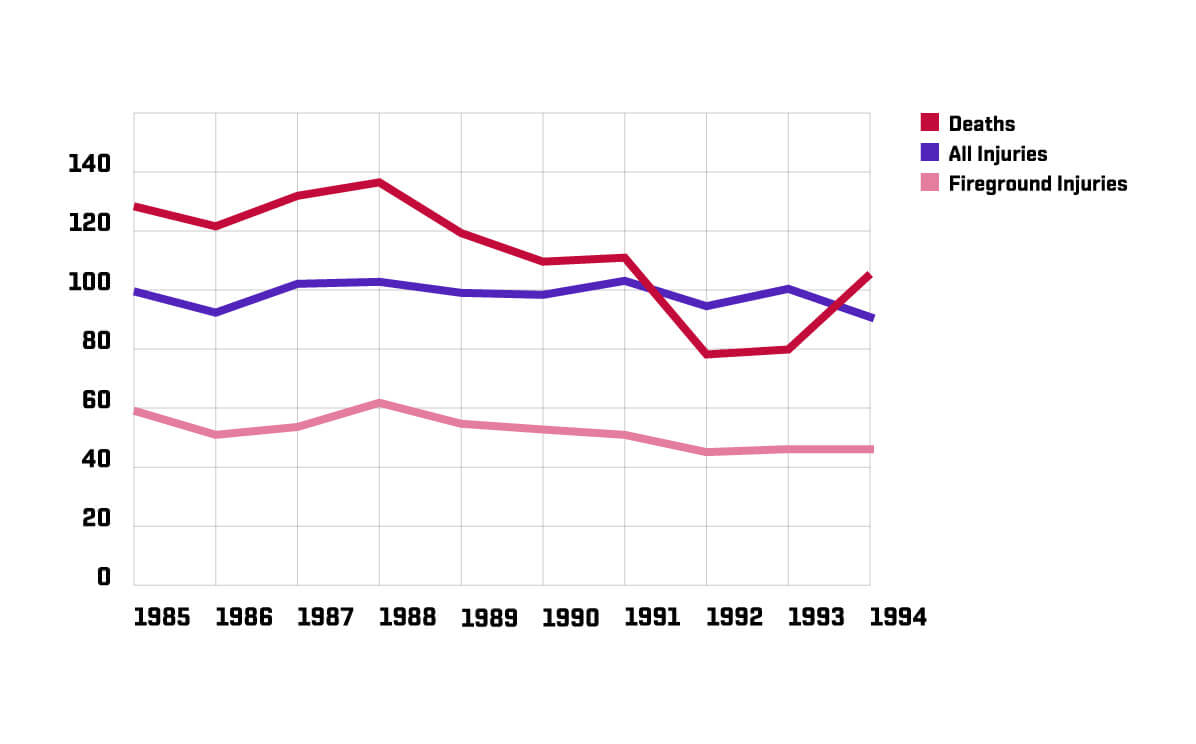

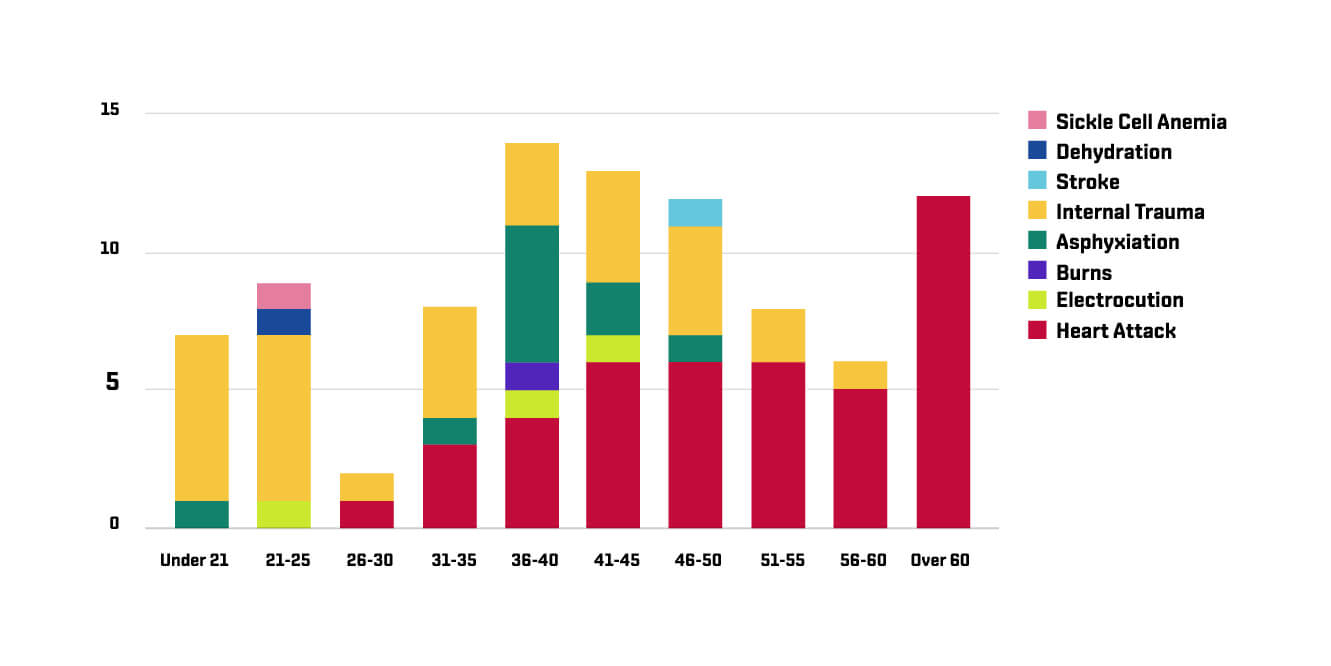
Figure 3: Age and Cause of Death (1996)

Four Studies make the case
Studies examining firefighters’ cardiac responses have focused on the extraordinary elevations in heart rates when responding to an alarm and during an emergency; James Barnard and Henry Duncan compiled one of the earliest of these reports, published in 1975.4 They studied higher-than-normal occurrences of ischemia, or reduced blood supply to the heart, in firefighters undergoing near-maximum exercise. They hypothesized that the “sudden exercise without warm-up” as well as thermal stress and inhaled pollutants, are partially responsible for ischemia. Their data, compiled on 35 Los Angeles firefighters over 24 hours and 189 alarms, measured heart rates response to varying situations.
The study found that between 15 and 30 seconds after the alarm, heart rates increased by 47 beats per minute on average, with the range increasing 12 to 117 beats per minute. One minute after the alarm, while on the truck, heart rates remained about 30 beats higher than normal; they ranged from an extra 1 to 80 beats per minute. Variations among individuals, even for the same person responding to different alarms, were noted (see figure 4). Personal variance was attributed to the type of alarm and rest factor of the individual. For night alarms, it seems that the more times one is roused from sleep by an alarm, the higher the heart rate elevation each successive time.
A follow-up study conducted in 1981 and published in the Journal of Occupational Medicine by Ilkka Kuorinka and Olli Korhonen on 22 firefighters in Helsinki, Finland, proved more astonishing. They found 61 beats per minute the “mean rise of the pulse rate from the initial level to the peak following the alarm.”5
Again, individual variation was evident, and there seemed to be a link between the increase in pulse rate and the activity engaged in before the alarm, sleeping, training, eating, etc. Within 15 seconds, the average heart rate would jump 61 beats.
A third study of 10 career firefighters, published in the Journal of Medicine in 1992, volume 34, examined the relation between heart rate response and cardiovascular fitness. By comparing oxygen consumption (VO2) during firefighting to a predetermined base level (VO2 Max, derived by running the subject on a treadmill until exhaustion) examiners could look closely at how hard the heart must work. The study found that in actual emergencies, the average heart rate was 157, or 88 percent of the maximum sustainable heart rate per individual.6


A similar study by J.E. Manning and T.R. Griggs showed heart rates increased to 70-80 percent of the maximum within the first minute and remained at 80-100 percent until the fire was out. This proved that once firefighters begin operating at such a high capacity any further encumbrance, such as heavy lifting, will further increase stress and reduce heart efficiency.7
Our professional lives are characterized by periods of relative inactivity punctuated rapidly by the sound of the Klaxon, often lasting for extended periods. We perform at or near maximum heart rate on a moment’s notice. It’s difficult to tell how much of this alarm-caused heart rate is physical and how much is psychological:findings are inconclusive. A portion of this jump may be caused by running to the truck, as hypothesized in the Helsinki study, but this activity seems unable to account for the extreme increase in heart rate and stress. Jogging for exercise, even for much longer periods of time, doesn’t produce nearly as high or as quick a jump in heart rate.8
Rather, as Kuorinka asserts, “the fireman’s (alarmed) states closely resembles a psychophysiological alarm reaction with fight or flight responses.”9 The ear-piercing sound of sirens, blinding flashes of strobe lights and the peril of dangerous traffic maneuvers compound stress, encouraging the body to release adrenaline and supercharge the nervous system.
The elevation of core body temperature associated with many firefighting tasks also stresses the heart. We operate under extremes, often in unbearable heat, in full protective gear and SCBA, compounded by tasks like climbing a ladder, rescuing a victim or holding a charged line while fire billows toxic smoke. Even in conditions much easier than these, firefighters experience significant elevations in core temperatures. For instance, an increase in core temperature while in turnout gear in moderate heat was linked with 5 percent decrease in plasma in a study by H.W. Duncan, et al. This decreases raises blood pressure and causes dehydration of the body’s tissues. Data suggested the volume decrease would have been greater had subjects worked for more than 15 minutes if the conditions had been as strenuous as fireground operations.10
Repeated exposure to carbon monoxide (CO) is another component. Breathing CO increases the amount of carboxyhemoglobin in blood, preventing oxygen from binding to the hemoglobin molecules in red blood cells, decreasing the amount of oxygen in the blood.11
At the time a firefighter is near maximum exertion, blood, heart and brain scream for oxygen. Lee Guidotti reported in 1992 Occupational and Environmental Health article that firefighters are at greater risk of ischemic myocardial injury due to carbon monoxide levels, or elevated circulating catecholamines (stress-related-chemicals).
Barnard concurred, saying repeated exposures to such pollutants may correlate with a higher incidence of ischemia in firefighters. CO exposure also seems to reduce the threshold for chest pain, also referred to as angina, which is a temporary lack of blood supply to the heart. Angina causes weakness and shortness of breath, and though it usually only mimics the symptoms of a heart attack, it can be a precursor to one.13 Long-term effects remain under debate, but it seems certain the effects cannot be positive.
The cardiovascular system gears up for physical activity at the sound of the Klaxon, but often no activity takes place. When an emergency worker’s body primes for battle and doesn’t follow through, the results are harmful.14
This repeated cycle, combined with the other exertions, place extreme stress on the heart and could result in myocardial ischemia. While normally insignificant, it’s the most commonly found cardiac condition in firefighters, usually accompanied by a rapid increase in heart rate. It signals a reduced blood supply to the heart; happening only occasionally in the non-firefighting population, this situation usually does no harm. The preparation for maximal exertion when no such effort takes place, or even maintaining the high level of heart rate for long periods of time, is particularly suspect where we are involved. Barnard supports this hypothesis, saying excessive catecholamines, hormones released during stress, may lead to the premature hardening of the arteries (atherosclerosis).15
Specific Risk Factors
Does the perceived gung-ho attitude of less-experienced firefighters evoke a higher increase in heart rate than in more experienced crews? Neither the Barnard nor the Helsinki study found substantial correlation.
One might suspect that out-of-shape firefighters would experience higher pulse rates after an alarm sounds than their fitter counterparts. But the Helsinki study found fitter firefighters actually had higher peaks. The authors attributed this partly to the ability of the fitter firefighters to get to the trucks more quickly, but they show no evidence to support this notion. It simply may come down to the individual response to an alarm.
Two studies questioned what effect the type of alarm system had on firefighters’ conditioned response. The Helsinki study suggested the Klaxon should “not strive for a physiological alarm reaction, but should be more informative.”16 Barnard and Duncan also questioned the alarm system, asking whether there was a difference between the old fashioned bell and the modern tone system. Both studies content that we know little about the impact of Klaxons, and that we could gain much by studying alarm systems further.
So many questions remain unanswered about cardiac responses to firefighting, in part, because of the variables that are hard to isolate in a true emergency. As Mark Sothmann pointed out in a Journal of Medicine article: “Although simulations generally are validated to replicate the type of tasks firefighters perform, at present there is little information on the comparability of simulations and actual emergencies in terms of intensity or duration of cardiorespiratory response.”17
Clearly, more studies on this subject are imperative. Health issues faced by firefighters, particularly those cardiac in nature, demand our attention.
About the Author
Garrett Law is a senior at Harvard College, majoring in history of science. He undertook this project as a research paper for a human physiology class. He is currently writing his senior thesis on fire sprinkler technology and development. Born in Sherrill, N.Y., he has been a firefighter with the Sherrill Kenwood Volunteer Fire Department for four years and a member of the ambulance crew this past year. He is a fourth-generation firefighter who is rebuilding a 1943 GMC pumper he bought when he was 13.
Sources
- “1996 Firefighter Injury Report.” NFPA Journal, November/December: p. 68, 1997.
- “Firefighter Fatalities in the United States in 1998.” United States Fire Administration. August: p 14, 1999.
- Ibid
- Barnard J, Duncan H: “Heart Rate and ECG responses of fire fighters.” Journal of Occupational Medicine. 17(4): p. 247, 1975.
- Kuorinka, I., Korhonen, O: “Firefighters’ reaction to alarm: Helsinki firefighters.” Journal of Occupational Medicine, 23(11): p. 764, 1981.
- Sothmann, Mark., with Saaupe K., Jasenof D., Blaney J. “Heart Rate Response of firefighters to Actual Emergencies; Implications for Cardiorespiratory Fitness.” Journal of Medicine. Vol. 34(8) p 797, 1992.
- Manning J, Griggs. T: “Heart rates in fire fighters using breathing equipment; similar near-maximal exertion in response to multiple work load conditions.” Journal of Occupational Medicine.” 25: pp. 215-218, 1983.
- Kuorinka et al. p. 764.
- Kuorinka et al. p. 762.
- Duncan H., Gardner G., Barnard J: “Physiological responses of men working in fire fighting equipment in the heat.” Ergonomics. 22: pp. 521-527, 1979.
- Lovett, E. Harvard University science teaching fellow in cardiology: Interview: April 12, 1998.
- Guidotti L: “Human factors in firefighting: ergonomic, cardiopulmonary, and psychogenic stress-related issues.” Occupational and Environmental Health. 64: p. 5, 1992.
- Ibid, p. 4.
- Gerspach J, Ferguson J: “Emotional Stabilization Program: From Red Lights to Recovery. Creative Interchange”, Huntington Beach, Calif. P. 42, 1981.
- Barnard, et al, p. 249.
- Kuornika et al, p. 764.
- Sothmann et al, pp. 798-799.
- Kuorinka et al, pp. 764-765.